The concept of intracranial pressure (ICP) and the regulation of its components, brain, blood, and cerebrospinal fluid (CSF), can be traced back to 1783 with Alexander Monro’s observations on the structure and function of the nervous system1. He noted that the amount of blood inside the skull should remain stable in normal and pathological conditions because the brain is nearly incompressible. He believed that in cases where fluid is secreted from blood vessels, a similar amount of blood would be pressed out of the cranium to compensate for the effused matter.
George Kellie, a former student of Monro, further supported the doctrine through publication of papers in 18242 on post-mortem examinations of two individuals who died during a winter storm. He stated that the circulation within the head is of a unique nature because the brain, which is little compressible, is contained within a rigid and unyielding skull.
He argued that a force must always be operating to maintain the plenitude of the vascular system within the head, and it’s not conceivable how any portion of the circulating fluid can ever be withdrawn from the cranium without an equivalent replacement.
Finally, in 1846, Burrows made modifications to the hypothesis in his book “On the disorders of the cerebral circulation”3. He posited that while cerebral blood volume may vary, it would only be to the benefit or detriment of brain and CSF volumes.
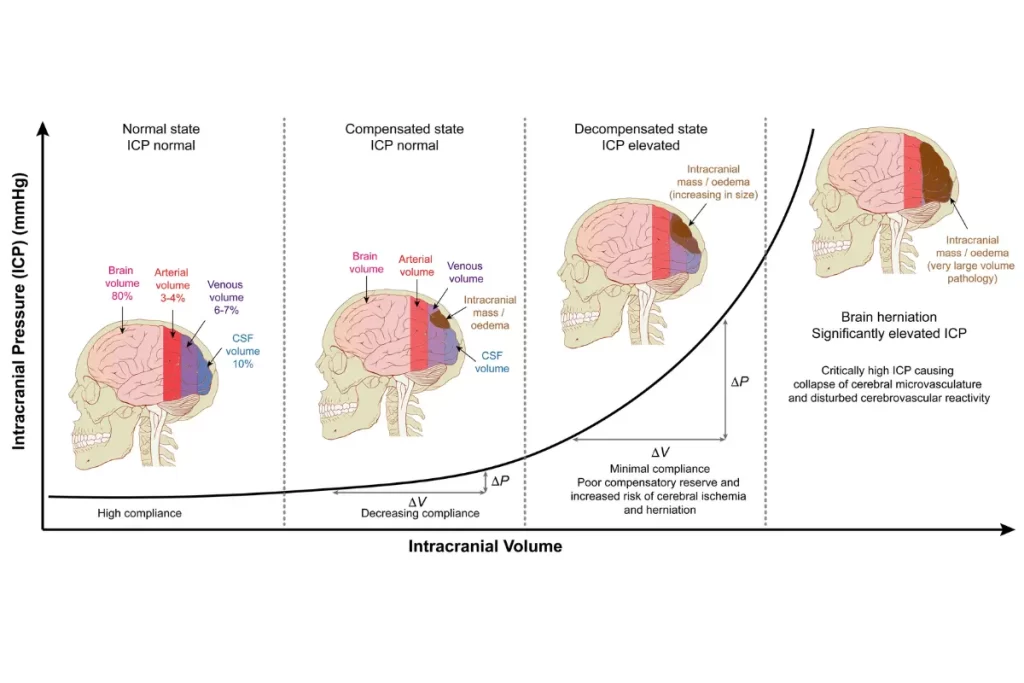
Together, these observations and modifications led to the formation of the Monro-Kellie doctrine, which states that the sum of volumes of brain, CSF, and intracranial blood is constant, and that an increase in one will result in a corresponding decrease in one or both of the other two. This hypothesis provides a basic understanding of ICP and its regulation, and is essential for the diagnosis and management of various neurological disorders.
The Monro-Kellie hypothesis states that the cranial vault is an enclosed space with limited volume, and the contents within this space – brain, blood, and CSF – exist in a state of dynamic balance. According to this hypothesis, any increase in the volume of one of the components within the cranial vault will result in a corresponding increase in ICP.
The production and absorption of CSF play a significant role in regulating ICP. An increase in CSF production or a decrease in its absorption can lead to an increase in ICP. Additionally, the volume of blood within the cranial vault also affects ICP, as any increase in blood volume due to factors such as increased heart rate or blood pressure, or due to bleeding, can result in an increase in ICP.
Brain edema, or swelling of brain tissue, is another factor that can lead to increased ICP. This can occur as a result of injury, infection, or other pathological conditions. When brain tissue swells, it increases the volume within the cranial vault and leads to an increase in ICP. Brain tumors can also increase ICP by occupying space within the cranial vault, leading to an increase in ICP and, in some cases, compressing adjacent brain tissue and causing neurological symptoms.
In summary, the Monro-Kellie hypothesis provides a straightforward way of understanding ICP and its regulation. By recognizing the relationship between brain, blood, and CSF within the cranial vault, healthcare providers can diagnose and treat conditions that affect ICP more effectively.
References:
1. Monro, A. Observations on the Structure and Functions of the Nervous System, Illustrated with Tables. Lond Med J 4, 113–135 (1783).
2. Kellie, G. An Account of the Appearances Observed in the Dissection of Two of Three Individuals Presumed to Have Perished in the Storm of the 3d, and Whose Bodies Were Discovered in the Vicinity of Leith on the Morning of the 4th, November 1821; with Some Reflections on the Pathology of the Brain: Part I. Trans Med Chir Soc Edinb 1, 84–122 (1824).
3. Sir, B., George. On disorders of the cerebral circulation: and on the connection between affections of the brain and diseases of the heart. (Longman, Brown, Green, and Longmans, 1846).